A Heartfelt “Welcome Home”: Honoring Our Veterans in Community
With deep gratitude, TRU Community Care thanks everyone who made our Veteran Lunch & Military…

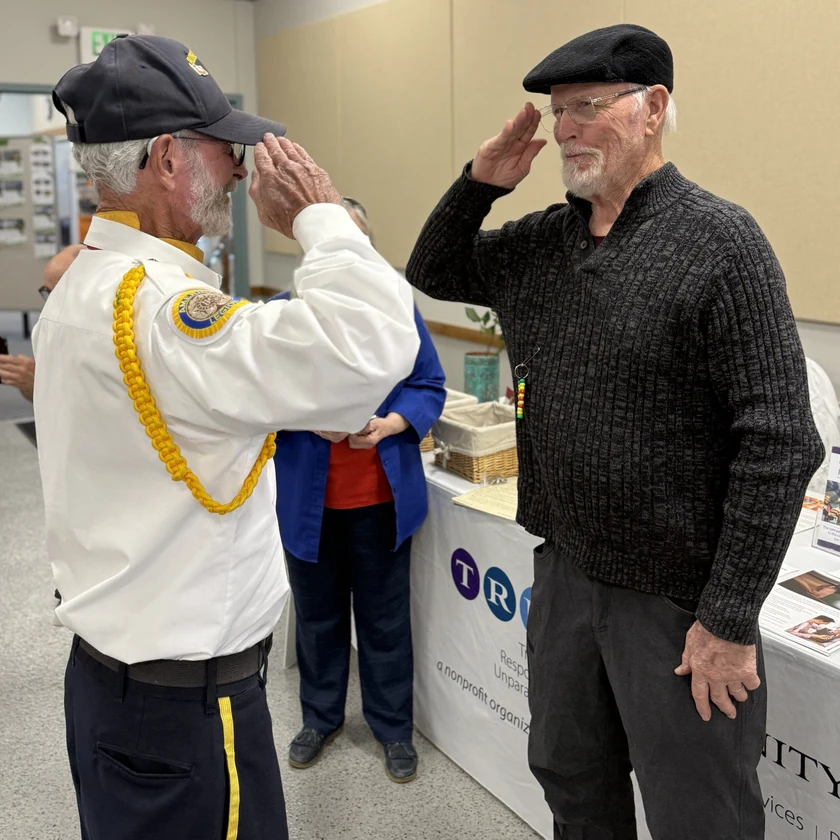
Veteran Lunch and Recognition Ceremony
Apex Community Recreation Center, Arvada TRU Community Care and Apex Park and Recreation District invite…

Lights of Life Remembrance Service Brings Community Together
Last month, TRU Grief Services and dedicated volunteers hosted the annual Lights of Life Remembrance…

The Power of Compassion: A Hospice Nurse’s Impact Goes Global
As an RN at TRU Community Care’s Hospice Inpatient Unit, Justin Raff’s days are filled…

Innovative Care for Rural Communities
by Rachel Stackhouse, TRU Clinical Educator If you reside in or travel to remote regions…

Empathy versus Compassion in Healthcare
by Rachel Stackhouse, TRU Clinical Educator There’s a concept I’ve been rolling over and over…

Benefits to Starting Hospice Sooner Rather than Later
There’s no doubt, the mention of hospice brings up ideas for people that often they’d…